
By Rob Knies, Managing Editor, Microsoft Research
Fourteen to 15 months—that’s the average prognosis for patients with glioblastoma, the most aggressive type of malignant glioma, according to Dr. Patrick Y. Wen, clinical director of the Center for Neuro-Oncology at the Dana-Farber Cancer Institute.
“These,” Wen told The New York Times in May 2008, “are unfortunately aggressive tumors.”
Microsoft research podcast

What’s Your Story: Lex Story
Model maker and fabricator Lex Story helps bring research to life through prototyping. He discusses his take on failure; the encouragement and advice that has supported his pursuit of art and science; and the sabbatical that might inspire his next career move.
Wen was quoted in a story announcing that U.S. Sen. Edward M. Kennedy had been diagnosed as having the brain tumor. Fifteen months and a few days later, Kennedy was dead.
“We know very little about what causes particular people to develop these devastating tumors, yet they are responsible for more years of lost life than almost any other adult cancer. They can cause paralysis, seizures, memory impairment, and even rob the patient of their personality and intellect,” says Antonio Criminisi (opens in new tab), senior researcher at Microsoft Research Cambridge (opens in new tab), who has been working with physicians from Cambridge University Hospitals. “Even when surgeons remove the tumor, it’s very likely that this type of tumor will reoccur somewhere else in the brain. There’s only so much brain you can remove.”
Criminisi and research partner Darko Zikic hope to provide new software tools to help surgeons and oncologists optimize treatment for these patients. The two are among the 10 authors of a paper entitled Decision Forests for Tissue-Specific Segmentation of High-grade Gliomas in Multi-channel MR (opens in new tab), which will be presented in Nice, France, during MICCAI 2012 (opens in new tab), the 15th International Conference on Medical Image Computing and Computer Assisted Intervention, scheduled for Oct. 1-5.

Image of a segmented glioblastoma in 3-D.
The goal of the project, supported by Microsoft Research Connections (opens in new tab) and being developed jointly with doctors at the Addenbrooke’s Hospital in Cambridge, is to delineate high-grade gliomas and individual tissue components automatically and reliably in 3-D magnetic-resonance-imaging (MRI) scans. Integrating information from different types of MRI scans before surgery is a complex, time-intensive process, yet that information can provide vital information to assist a surgeon in planning the most appropriate form of surgery for a patient. After surgery, patients usually require radiation therapy and chemotherapy treatment, and the same tools can be used to help the oncologist plan treatment for the patient and assess how well treatment has worked.
“The long-term goals,” Zikic says, “are improving the clinical procedures and enabling research through the measurements we hope to enable.”
Stephen Price (opens in new tab) of Cambridge (U.K.) University Hospitals notes the value such research could deliver.
“If we ever want to get the research we are doing on advanced imaging of these tumors to get into clinical practice,” Price says, “we need tools that can perform tasks automatically. A busy clinician is not going to be able to spend time to segment an image, even if it is shown that the information you get from it will have an effect on the way patients are treated.”
The Microsoft researchers are working on two tools to assist surgeons and oncologists treating a patient with glioblastoma.
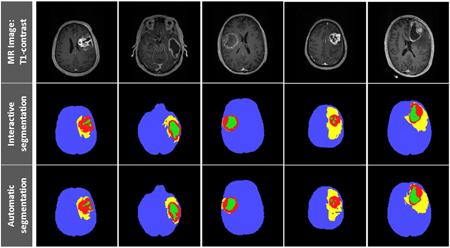
Examples of the interactive and automatic segmentation results for five patients.
The first tool provides a highly effective means of computer-assisted segmentation. Currently, physicians will take a magnetic-resonance scan of a brain and carefully draw an outline on each 2-D slice of the tumor and its constituent parts: areas of actively growing tumor, areas of tumor that have grown so fast that they have run out of nutrients and oxygen and are starting to die, and the area of brain surrounding the tumor that shows signs of swelling and inflammation. These manual segmentations are time-consuming and error-prone, yet it is vital to perform this step to get quantitative measurements of the 3-D shape of the tumor.
The technique the researchers are using could diminish dramatically this laborious process—to as brief as 15 minutes. Dr. Raj Jena (opens in new tab), a radiation oncologist based at Addenbrooke’s, has been assessing the system with some of his cases.
“Existing commercial systems can produce reasonable automatic segmentations of normal healthy anatomical structures,” he says. “However, segmenting a glioma is difficult, because the tumor can have such a varied appearance. The interactive segmentation is a very good way to avoid this problem. To segment a glioma for radiotherapy treatment normally takes me more than an hour, and with the interactive segmentation tool, I have achieved the same result in five minutes. This could be very beneficial for my patients by reducing the time they must wait to start radiation therapy after surgery.”
The second tool on which the team is working could be even more helpful, by providing fully automatic, 3-D tumor delineation.
“With our interactive tool, we have all these regions of interest that are already segmented,” Zikic says. “We then can apply machine-learning techniques to learn from these manual labelings how, given a new MR image, the segmentation should look.”
The researchers have devised an algorithm to replicate the manual annotations—and to generalize on a previously unseen patient-data set. The system can be trained to compute the segmentation accurately and efficiently. The technique used to segment the tumors into their component parts is a discriminative approach based on the use of decision forests using context-aware spatial features. Individual tissue types are classified simultaneously, and the results are computationally efficient, with low model complexity.
The tools have been evaluated quantitatively using a labeled database of 40 multichannel magnetic-resonance images—believed to be the largest annotated database of its kind.
“We ran quantitative analysis,” Zikic says, “that shows that these results are very good compared to what was previously reported in the literature.”
The segmentation is not perfect. It still needs to be confirmed by a physician. But the surgeons and oncologists working with the team are really excited about the results. Jena explains why.
“For the first time in 40 years, we have new drug treatments that are showing promising results for patients with glioblastoma,” he says. “These new drugs act on specific mechanisms within the tumor, and their effects can be quite subtle. We need to be able to look at the scans of a patient using different imaging techniques, taken at different points in the patient’s treatment. In this way, we can start to pick out the earliest subtle changes that tell us whether a treatment is working for a particular patient.
“The old-fashioned techniques of measuring a tumor to see if it is bigger, smaller, or the same size are just not good enough. We have always understood that full quantitative assessments of the tumor could yield important information, but we have lacked the tools needed to do this in the clinic.”
The researchers, understandably, are pleased to hear such comments.
“I am excited when I hear from my medical colleagues about how these tools could be used,” Criminisi says. “Perhaps a patient reviewing his images with his surgeon might want to take a little extra risk and have a little more of the brain removed, which we know has already been damaged, to improve the prognosis and increase his or her remaining lifespan. Perhaps another patient who is struggling with the effects of chemotherapy might be helped by knowing very early in his treatment that the tumor is showing signs of response: It might just give him the extra drive needed to keep going with treatment.”
Interestingly, Criminisi sees this work, while largely focused on fighting brain tumors, is in keeping with the computer-science work Microsoft Research Cambridge pursues.
“I don’t see our group as a purely medical-imaging research group,” he states. “It’s more machine-learning, computer-vision work. We use the analysis of medical images, which is tough and a real problem, as an opportunity to do great computer-science research.”
Joining Criminisi and Zikic as authors of the MICCAI paper are Ben Glocker, Ender Konukoglu, and Jamie Shotton (opens in new tab) of Microsoft Research Cambridge; Çağatay Demiralp (opens in new tab), a 2011 intern at that lab; and Jena, Price, Dr. Owen Thomas, and Tilak Das of Cambridge University Hospitals.
Still, as both Zikic and Criminisi stress, providing high-quality initial estimates for interactive treatment planning does have certain rewards.
“What gets me out of bed every morning,” Criminisi says, “is the idea that what we do can make the lives of very unfortunate people a bit less sad, maybe a little bit longer, and perhaps improve a little bit their quality of life.”



